Intraventricular baclofen and bilateral pallidotomy in a pediatric patient with acquired generalized dystonia and refractory status dystonicus: illustrative case
DOI:
https://doi.org/10.46900/apn.v7i3.312Keywords:
Selected:Intraventricular baclofen, bilateral pallidotomy, dystonia, status dystonicusAbstract
Background: Status dystonicus (SD) is a life-threatening emergency in pediatric patients with severe dystonia, often requiring intensive care. Surgical interventions, such as deep brain stimulation, intrathecal baclofen (ITB), or pallidotomy, are considered for refractory cases, but evidence for intraventricular baclofen (IVB) and bilateral pallidotomy (BP) in children is limited. We report a novel combined approach using IVB followed by BP in a 3-year-old boy with refractory SD secondary to hypoxic-ischemic encephalopathy.
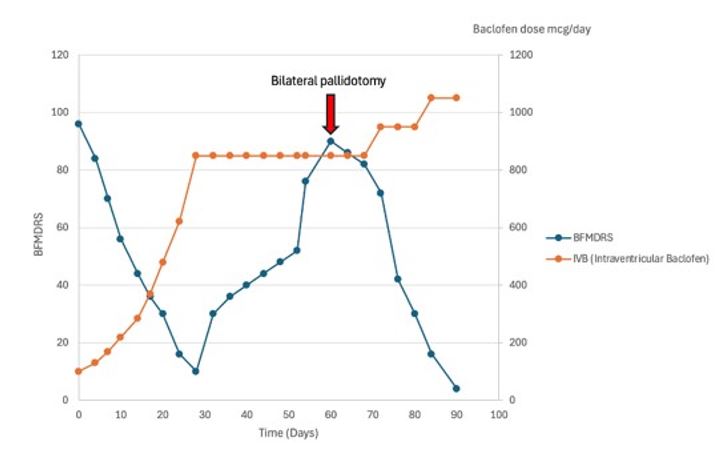
Case Description: A 3-year-old male developed SD and spastic quadriparesis following cardiorespiratory arrest due to airway obstruction. Despite aggressive medical management (levodopa, clonazepam, tetrabenazine, oral baclofen, sedatives), SD persisted, requiring prolonged mechanical ventilation. An ITB test (100 mcg) reduced the modified Ashworth scale from 5 to 3 and dystonic episodes from 8 to 2/day. IVB was placed via a third ventricle catheter with a pump delivering 100-1050 mcg/day, achieving spasticity control but fluctuating dystonia response. Due to recurrent SD, poor prognosis, and malnutrition, BP was performed using stereotactic microelectrode guidance and radiofrequency lesions (80°C, 60s). Postoperative MRI confirmed precise pallidal lesions. The patient achieved full SD resolution, was weaned from ventilation, and stabilized at home with tracheostomy and gastrostomy.
Conclusions: Bilateral pallidotomy and IVB should be considered in the treatment of refractory SD, particularly for patients with contraindications for DBS and concurrent severe spasticity. The literature review support this findings, providing an overview that can guide palliative management in similar cases. Further studies are needed to establish comprehensive guidelines for surgical management of SD in children.
Downloads
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Juan Camilo Arias-Angulo, Sebastián Ordóñez-Cure, Oscar Escobar-Vidarte, Lucely Ortega-Bolaños

This work is licensed under a Creative Commons Attribution 4.0 International License.

When publishing in Archives of Pediatric Neurosurgery journal, authors retain the copyright of their article and agree to license their work using a Creative Commons Attribution 4.0 International Public License (CC BY 4.0), thereby accepting the terms and conditions of this license (https://creativecommons.org/licenses/by/4.0/legalcode).
The CC BY 4.0 license terms applies to both readers and the publisher and allows them to: share (copy and redistribute in any medium or format) and adapt (remix, transform, and build upon) the article for any purpose, even commercially, provided that appropriate credit is given to the authors and the journal in which the article was published.
Authors grant Archives of Pediatric Neurosurgery the right to first publish the article and identify itself as the original publisher. Under the terms of the CC BY 4.0 license, authors allow the journal to distribute the article in third party databases, as long as its original authors and citation details are identified.