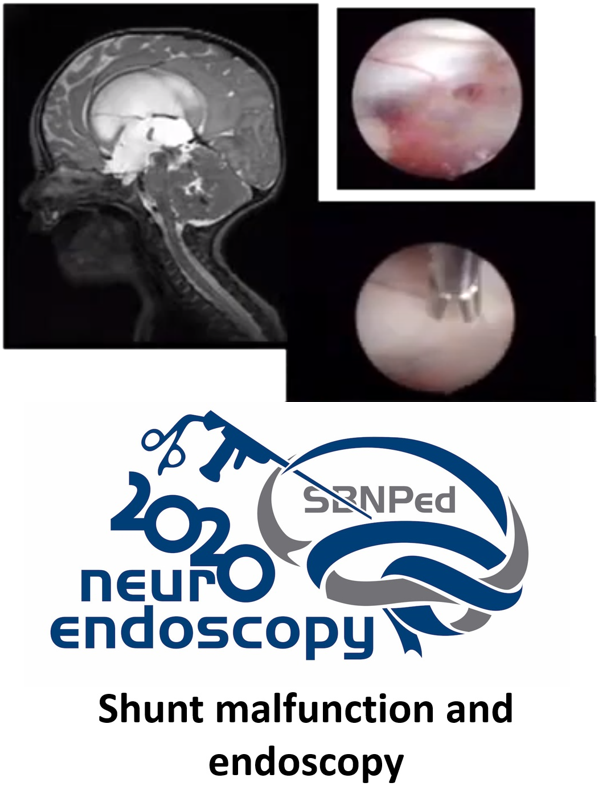
Shunt malfunction and endoscopy
DOI:
https://doi.org/10.46900/apn.v3i1(January-April).79Keywords:
Shunt malfunction, NeuroendoscopyAbstract
Objective:
Hydrocephalus is the most common neurological disease in pediatric neurosurgery.(1) The CSF shunts remains as the most common treatment choice for nonobstructive hydrocephalus worldwide, but shunt complications still the most common neurosurgical problem, especially in pediatric neurosurgery. Endoscopy and shunts are the way to treat hydrocephalus. Especially third ventriculostomy is the most effective treatment to obstructive hydrocephalus but shunt still the most important way to treat.(2, 3) Shunt malfunction is frequent and after so many years this is very important problem to the patients. Ventricular problem due to obstruction is responsible up to 72% of shunt problems.(4) The Shunt Trial Study showed that the overall shunt survival was 62% at 1 year, 52% at 2 years, 46% at 3 years, 41% at 4 years. The survival curves for the 3 differents valves were similar to those from the original trial and did not show a survival advantage for any particular valve.(5, 6) We still don´t have one perfect solution to hydrocephalus and shunt malfunction.
The major author described his experience in use endoscopy to evaluate and treat shunt malfunction and one new approach and way to evaluate this problem.
Results/Discussion:
The literature review was performed, and we found 84 articles when we used the keywords. Endoscopy has been one important way to treat and solve shunt problems. In obstructive hydrocephalus third ventriculostomy is the best way to treat these patients.(1-3)
The major author first described goals of endoscopy. First goal is safe catheter removal in surgical review, avoiding bleeding when removing catheter addressing all the adhesions on catheter. Second goal is put in optimal position the new catheter with pure endoscopy view or using neuronavigation systems that could help the endoscope system.(7, 8)
Optimal new catheter placement and optimal long-term catheter survival are especially important because most of the problems are due to ventricular problems. These good placements could avoid loculations and ventricular collapse with ependymal problems. Avoid new catheter malpositiitioning, you can use the endoscope to follow the old tract to insert the new catheter in one good position avoiding choroid plexus. Another situation is when you have small ventricles especially in slit ventricle syndrome.
The major author has been studied some causes to ventricular catheter obstruction. He noticed after some surgical reviews some ventricular ependymal inside catheter. Ventricular ependymal protrusions inside the catheter could cause intermittent occlusion.(8) Some endoscope views showed these protrusion and ependymal changes after intermittent increase and decrease of ventricular pressure. These protrusions correspond to catheter holes a secondary to suction. These protrusions could stuck in the holes in chronicle suction.(8) The major author reported one endoscopic evidence of overdrainage-related ventricular tissue protrusions that cause partial or complete obstruction of the ventricular catheter. He did a retrospective review in fifty patients underwent 83 endoscopic shunt revision procedures that revealed in-growth of ventricular wall tissue into the catheter tip orifices (ependymal bands), producing partial, complete, or intermittent shunt obstructions. Endoscopic ventricular explorations revealed ependymal bands at various stages of development, which appear to form secondarily to siphoning.(8)
How to minimize this overshunting? Anti siphon systems could help and decrease proximal shunt malfunction in some complex patients. The other problem is ventricular bleeding. The use of endoscope has been important tool to remove ventricular catheters, when you could see the adhesions.(9)
The use the endoscope could be particularly important to open loculations and cysts avoiding ventricular entrapment. Patients with ventricular cysts could need more than one catheter. The use of endoscopy to fenestrate the cyst could keep the patient with one catheter or without any shunt system.(10, 11)
Conclusion:
Shunt malfunction has a lot of possible causes, but a probably ventricular catheter problem is the most common situation. Choose appropriate endoscope rigid or flexible for each case could help to treat and avoid some of ventricular. Endoscopy could be one important tool to help the surgeon to understand and solve this dangerous situation to the patient. Ventricular wall protrusions are a significant cause of proximal shunt obstruction, and they appear to be caused by siphoning of surrounding tissue into the ventricular catheter orifices.
Downloads
References
2. Cinalli G, Cappabianca P, de Falco R, Spennato P, Cianciulli E, Cavallo LM, et al. Current state and future development of intracranial neuroendoscopic surgery. Expert Rev Med Devices. 2005;2(3):351-73.
3. Demerdash A, Rocque BG, Johnston J, Rozzelle CJ, Yalcin B, Oskouian R, et al. Endoscopic third ventriculostomy: A historical review. Br J Neurosurg. 2017;31(1):28-32.
4. Kestle J, Milner R, Drake J. The shunt design trial: variation in surgical experience did not influence shunt survival. Pediatr Neurosurg. 1999;30(6):283-7.
5. Drake JM, Kestle JR, Milner R, Cinalli G, Boop F, Piatt J, et al. Randomized trial of cerebrospinal fluid shunt valve design in pediatric hydrocephalus. Neurosurgery. 1998;43(2):294-303; discussion -5.
6. Kestle J, Drake J, Milner R, Sainte-Rose C, Cinalli G, Boop F, et al. Long-term follow-up data from the Shunt Design Trial. Pediatr Neurosurg. 2000;33(5):230-6.
7. Kraemer MR, Sandoval-Garcia C, Bragg T, Iskandar BJ. Shunt-dependent hydrocephalus: management style among members of the American Society of Pediatric Neurosurgeons. J Neurosurg Pediatr. 2017;20(3):216-24.
8. Kraemer MR, Koueik J, Rebsamen S, Hsu DA, Salamat MS, Luo S, et al. Overdrainage-related ependymal bands: a postulated cause of proximal shunt obstruction. J Neurosurg Pediatr. 2018;22(5):567-77.
9. Koueik J, Kraemer MR, Hsu D, Rizk E, Zea R, Haldeman C, et al. A 12-year single-center retrospective analysis of antisiphon devices to prevent proximal ventricular shunt obstruction for hydrocephalus. J Neurosurg Pediatr. 2019:1-10.
10. Zuccaro G, Ramos JG. Multiloculated hydrocephalus. Childs Nerv Syst. 2011;27(10):1609-19.
11. Piyachon S, Wittayanakorn N, Kittisangvara L, Tadadontip P. Treatment of multi-loculated hydrocephalus using endoscopic cyst fenestration and endoscopic guided VP shunt insertion. Childs Nerv Syst. 2019;35(3):493-9.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2021 Bermans Iskandar, Ricardo de Amoreira Gepp

This work is licensed under a Creative Commons Attribution 4.0 International License.

When publishing in Archives of Pediatric Neurosurgery journal, authors retain the copyright of their article and agree to license their work using a Creative Commons Attribution 4.0 International Public License (CC BY 4.0), thereby accepting the terms and conditions of this license (https://creativecommons.org/licenses/by/4.0/legalcode).
The CC BY 4.0 license terms applies to both readers and the publisher and allows them to: share (copy and redistribute in any medium or format) and adapt (remix, transform, and build upon) the article for any purpose, even commercially, provided that appropriate credit is given to the authors and the journal in which the article was published.
Authors grant Archives of Pediatric Neurosurgery the right to first publish the article and identify itself as the original publisher. Under the terms of the CC BY 4.0 license, authors allow the journal to distribute the article in third party databases, as long as its original authors and citation details are identified.